
 Idiopathic hypersomnia and narcolepsy types 1 and 2 have some similar and overlapping symptoms. For example, all of these disorders cause excessive daytime sleepiness and brain fog. Other symptoms are more common or less common in people who have these disorders.
Idiopathic hypersomnia and narcolepsy types 1 and 2 have some similar and overlapping symptoms. For example, all of these disorders cause excessive daytime sleepiness and brain fog. Other symptoms are more common or less common in people who have these disorders.
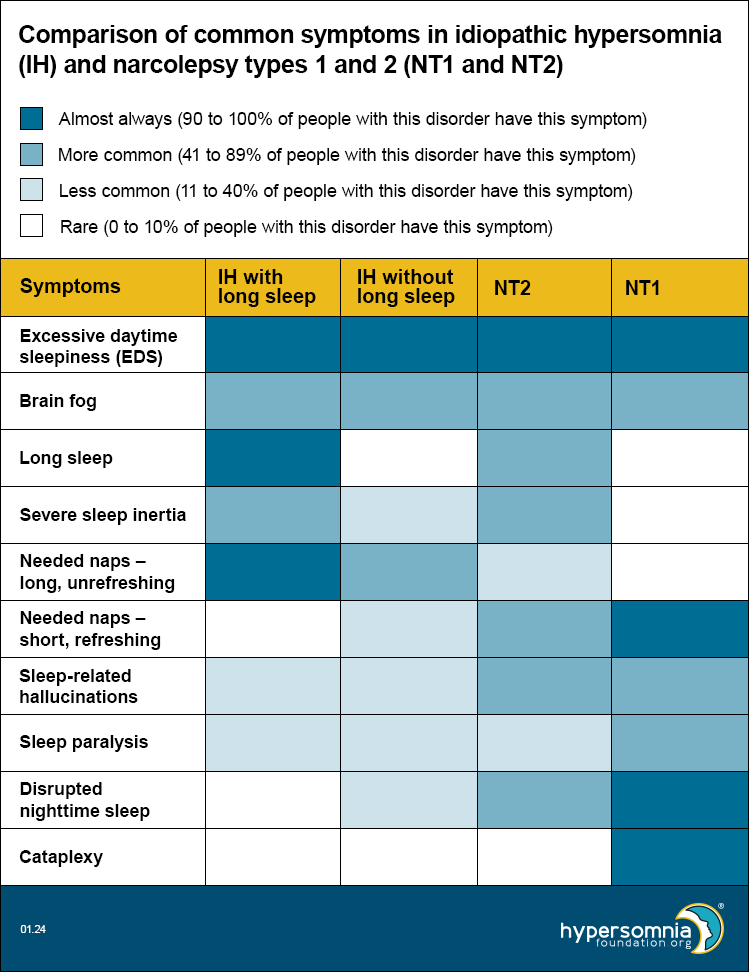
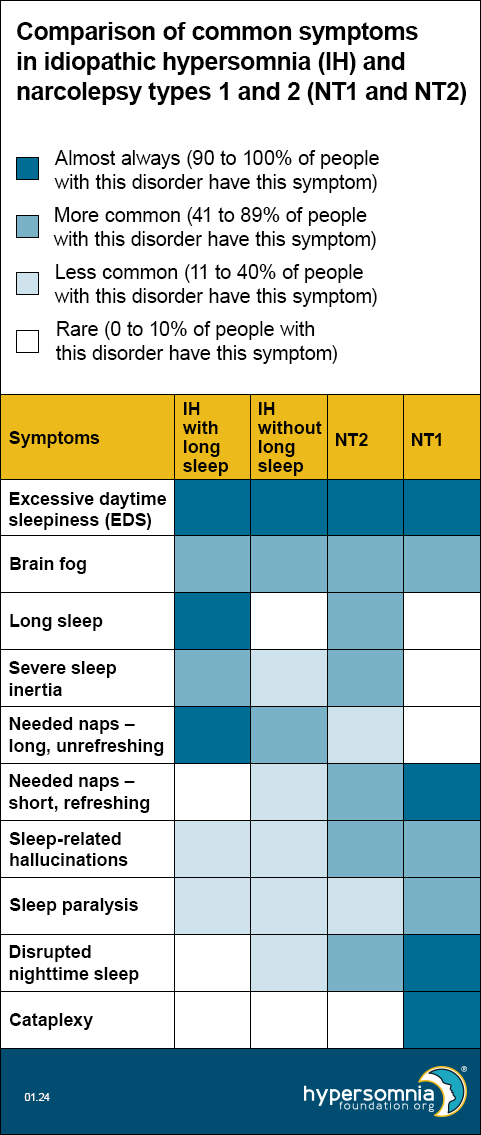
The table below compares how common certain symptoms are in:
- Idiopathic hypersomnia (IH) with long sleep
- IH without long sleep
- Narcolepsy type 2 (NT2)
- Narcolepsy type 1 (NT1)
This table can be helpful in thinking about which type of sleep disorder you may have. Because many researchers think IH without long sleep and NT2 may be the same disorder, we’ve placed them next to each other to help you compare them more easily.
The colors in the table show how common it is for people with that disorder to have that specific symptom. The legend tells you what each color means. For example, dark blue means people with that disorder almost always have that symptom. The numbers show what percent (how many people out of 100) of people have that symptom.
Refer your doctors to our web page for them: “Diagnosis, classification, symptoms, and causes of hypersomnias.”