Read about hypersomnia sleep disorders
such as idiopathic hypersomnia, narcolepsy types 1 and 2, and Kleine-Levin syndrome

such as idiopathic hypersomnia, narcolepsy types 1 and 2, and Kleine-Levin syndrome

On this page you’ll read about idiopathic hypersomnia (IH), including:
On this page you’ll read about narcolepsy type 2 (NT2), including:
On this page you’ll read about narcolepsy type (NT1), including:
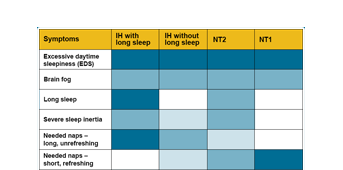
Find our table showing how common the symptoms are in each of these disorders.

On this page you’ll read about Kleine-Levin syndrome, including:

Sleep problems such as excessive daytime sleepiness and sleeping for 9 to 12 hours or more can be associated with many different health conditions. On this page you’ll find resources and a list of these health conditions.
Health terms can be hard to understand, and it can be helpful to learn the meaning of terms that you'll run into when reading and talking about hypersomnia sleep disorders. Find plain language definitions you’ll want to know if you’re living with a hypersomnia sleep disorder or supporting someone who does.